Understanding Infectious Bursal Disease virus diagnostic techniques
10 February 2025
There are several diagnostic techniques available for Infectious Bursal Disease (IBD) which can be very useful in poultry vets’ daily practice. However, to ensure their efficient use, it is crucial to know how to interpret them and what valuable information each of them provides us with. Understanding each of these diagnostic techniques well is one of the key points for prevention and control of the disease.
The laboratory diagnosis of Infectious Bursal Disease is useful for two main reasons. On the one hand, for detection of the aetiological agent that is causing an outbreak as the IBD virus does not always show clear signs of the disease and on the other hand, as a vaccination performance follow-up, that is to say, to assess whether the vaccine administered in a flock is working in the way it should and that the birds are responding properly to it.
When a Gumboro disease outbreak is suspected, the first step will always be to take an exhaustive evaluation of the chicks for a clinical diagnosis, along with a postmortem examination to detect lesions and signs compatible with IBDV. However, to really confirm which pathogen is causing the problem that has been detected , we must rely on laboratory techniques.
Clinical diagnosis is based on medical signs and reported symptoms. This is only useful for clinical IBDV, as subclinical IBDV will not cause any signs , and so is easily underdiagnosed. The severity of the signs will depend on the age, breed, virulence of the strain, etc. but in general, a clinical IBDV case can be described as follows:

All these detected changes can lead us to suspect a case of Gumboro. However, as mentioned above, for a final confirmation we must use laboratory techniques such as serology, molecular diagnosis and histopathology.
Serology is a widely used technique that aims to evaluate the response of the immune system (antibodies in blood serum) to pathogens or vaccines. The most widely used test is the enzyme-linked immunosorbent assay, also called ELISA, which is a test that detects and measures IBDV antibodies in the blood.
The main inconvenience is that it cannot directly differentiate the type of strain that is present on the farm and on some occasions the interpretation might be difficult as some IBDV field strains do not lead to higher levels of titres compared to vaccines.
It must be borne in mind that each commercial ELISA kit can be very different in terms of results and interpretation, mainly due to the type of antigen inserted and the lower or higher range of detection. So, when referring to ELISA titres, it is important to specify which kit has been used to analyse the sera.

For direct detection of an antigen, the most widely used technique is molecular diagnosis: PCR for the detection of a positive sample and sequencing for the detection of the specific strain. This technique allows us to identify a target genetic sequence of DNA or RNA.
PCR is a molecular technique that amplifies a small fragment or even the whole genome of a microorganism present in a sample. In the case of Gumboro virus, the amplified gene is the VP2 gene since it is the most immunogenic protein, located on the surface of the virus. However in recent years, a new genotypic classification of IBDV based on VP1 and VP2 proteins has been proposed and is becoming more commonly used.
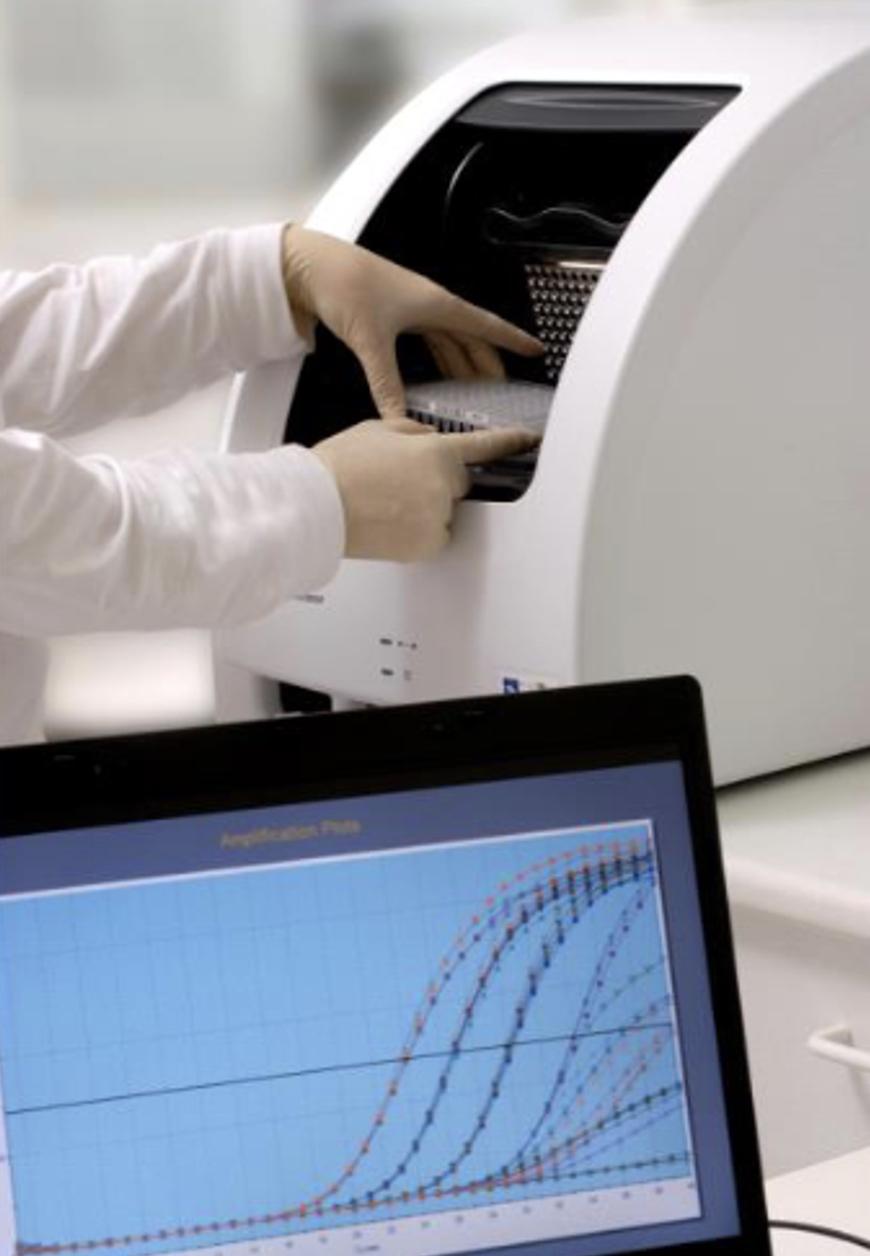
The aim of the PCR is to generate millions and millions of copies of this specific gene in order to be able to detect a very small amount of the virus present in the sample. After repeating different cycle temperatures, PCR doubles and increases the number of copies of this genetic material, at the end generating millions of copies of the initial amount.
The Ct value is the number of cycles that a sample needs to be detected as positive, and it is inversely proportional to the initial amount of genetic material present in the sample. The higher the Ct value, the higher the number of cycles this sample needs to be detected as positive, so the lower is the amount of genetic material present in this sample. This gives us a semi-quantitative way of quantifying the amount of genetic material in the sample.
The bursa of Fabricius is the tissue of choice for the isolation of IBDV because it contains the highest virus titre and persists for longer, as the virus replicates in B-lymphocytes present in the organ. Sampling is performed in the bursas by using FTA cards, which are sent to the laboratory for amplification of the genetic material.
If the sample is positive, it will then be sent for virus typing to determine which specific type of Gumboro virus is present. The sequences obtained are then analysed using different software to compare them with sequences published in a database.
Histopathology is a laboratory technique for evaluation of microscopic lesions. In the case of Gumboro disease, it is commonly used to evaluate lesions present in the bursa of Fabricius. It is important to remark that this diagnosis technique provides information about Infectious Bursal Disease compatible lesions, but it does not confirm the causative agent or the virus that is present. It is useful in order to know the virulence of a specific strain, to compare the effect of IBDV vaccines and field strains (or to compare different types of vaccines) and to estimate the momentum of the infection at the time the sample was taken (acute or chronic phase).
Histopathology is also useful to score the lymphoid depletion caused by live IBD field viruses and vaccines. The most recognized method is the European Pharmacopoeia lesion scoring scale, that evaluates the replication level of live vaccine strains in the bursa, based on lymphoid depletion only, not other inflammatory signs. This scoring ranges from 0 (no lymphoid depletion) to 5 (100% of follicles show nearly complete lymphoid depletion). In practice, this histopathological evaluation of the bursa is done from 28 (acute phase of the infection) to 35 days of age (chronic phase).
It is important to bear in mind that there are other scoring scales, so it should be clear which scale is used by the laboratory where the samples are sent to be analysed. The vaccine that is used should also be taken into account, as only live vaccines reach the bursa: